

Background: The clinical management of ITP has been evolving. Thrombopoietin receptor agonists (TPO-RAs) have become widely utilized as subsequent treatments, and the 2019 ASH guidelines recommend their use over rituximab to achieve a durable response.
TPO-RAs eltrombopag (ELT) and romiplostim (ROMI) have been FDA approved for over a decade with a well demonstrated efficacy profile. ELT, an oral medication, must be administered two hours prior to or four hours after meals containing polyvalent cations such as calcium or magnesium to mitigate clinically relevant effects on the pharmacokinetic profile (ELT prescribing information). Additionally, ELT carries a boxed warning for hepatoxicity that requires monitoring. ROMI, an injectable, is typically administered in a health care practitioner's office weekly which may be challenging for some patients (Pts).
Avatrombopag (AVA) is an oral TPO-RA approved in 2019 for Pts with ITP. In clinical trials, AVA rapidly increased platelet count (PC) (5 days) and maintained it in the target range (50 to 150×109/L) with chronic dosing. Further, it has an exposure-adjusted safety profile generally comparable to placebo with no boxed warning for hepatotoxicity. AVA does not chelate polyvalent cations; therefore, it is administered with food and without restrictions regarding meal composition. A high proportion of Pts (~90%) respond to AVA; but limited information is available regarding the durability of response over time utilizing clinically relevant loss of response definitions.
Aims: To understand the duration of initial response with AVA and the overall percent of treatment days a response level PC was achieved in responding Pts.
Methods: A 6-month, multicenter, randomized, double-blind, Phase 3 study enrolled 32 AVA and 17 placebo-treated Pts with ITP. The study design included a 6-week study drug titration period, 12-week concomitant ITP medication reduction period, and an 8-week maintenance period. The primary endpoint was the median number of cumulative weeks of PC response (PC ≥50,000/µL) over the course of the study without rescue medication. Pts receiving rescue medication during the study were deemed to be non-responders for the remainder of the study.
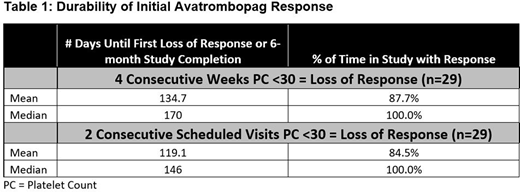
For this post-hoc analysis, we analyzed how many days it took for responding AVA Pts (n=29) to experience their first loss of response (LOR) or reach core study conclusion. After the initial PC ≥50,000/µL was noted, we also examined the percentage of remaining treatment time that initial response was maintained. Response was defined as the first time achieving a PC ≥50,000/µL. LOR was defined as a Pt experiencing a PC <30,000/µL for 4 consecutive weeks (LOR-4wk), or in a more conservative manner, Pts experiencing a PC <30,000/µL on 2 consecutive scheduled visits (LOR-2vis) [visits were weekly or biweekly depending on the phase of the study with 21 visits occurring over 26 weeks]. When a LOR was observed, the date of the first PC <30,000/µL was used for subsequent calculations with a return of response defined as a PC exceeding ≥30,000/µL again. Pts who required rescue therapy (n=6) were included in the analyses and the first date of administration was used for the LOR date. Pts requiring either corticosteroids (n=4) or IVIg (n=1) as rescue therapy were considered non-responders for a minimum of 8 weeks and Pts receiving a platelet transfusion (n=1) for a minimum of 1 week.
Results: 72.4% (21/29) and 55.2% (16/29) of AVA responsive Pts never experienced a LOR-4wk or LOR-2vis, respectively. The median number of days until responding Pts experienced their first LOR-4wk, discontinued treatment, or completed the 6-month study was 170 (mean 134.7) and 146 (mean 119.1) for the LOR-2vis analysis. Pts maintained their initial response on average for 87.7% (median 100%) of their remaining time in the study for LOR-4wk and 84.5% (median 100%) for LOR-2vis analyses, with Pts often losing response only briefly when noted. Pts requiring rescue therapy often returned to a response level PC and remained in the 6-month study for approximately 5 months following their initial response.
Conclusions: These data suggest that the initial response to AVA is stable and durable with up to 72.4% of Pts never experiencing a LOR, even with the planned objective of reducing the use of baseline concomitant ITP medications during the study. In those pts experiencing a LOR, many ended up achieving response level PCs again without a subsequent LOR.
Wojdyla:Dova Pharmaceuticals: Current Employment. Vredenburg:Dova Pharmaceuticals: Current Employment. Jamieson:Dova Pharmaceuticals: Current Employment. Gernsheimer:Amgen Corporation: Consultancy, Honoraria; Novartis: Consultancy; Cellphire: Consultancy; Rigel Corporation: Consultancy, Research Funding; Principia: Research Funding; Sanofi: Consultancy; Vertex: Consultancy; Dova Pharmaceuticals: Consultancy.

